
Here's what we built instead.
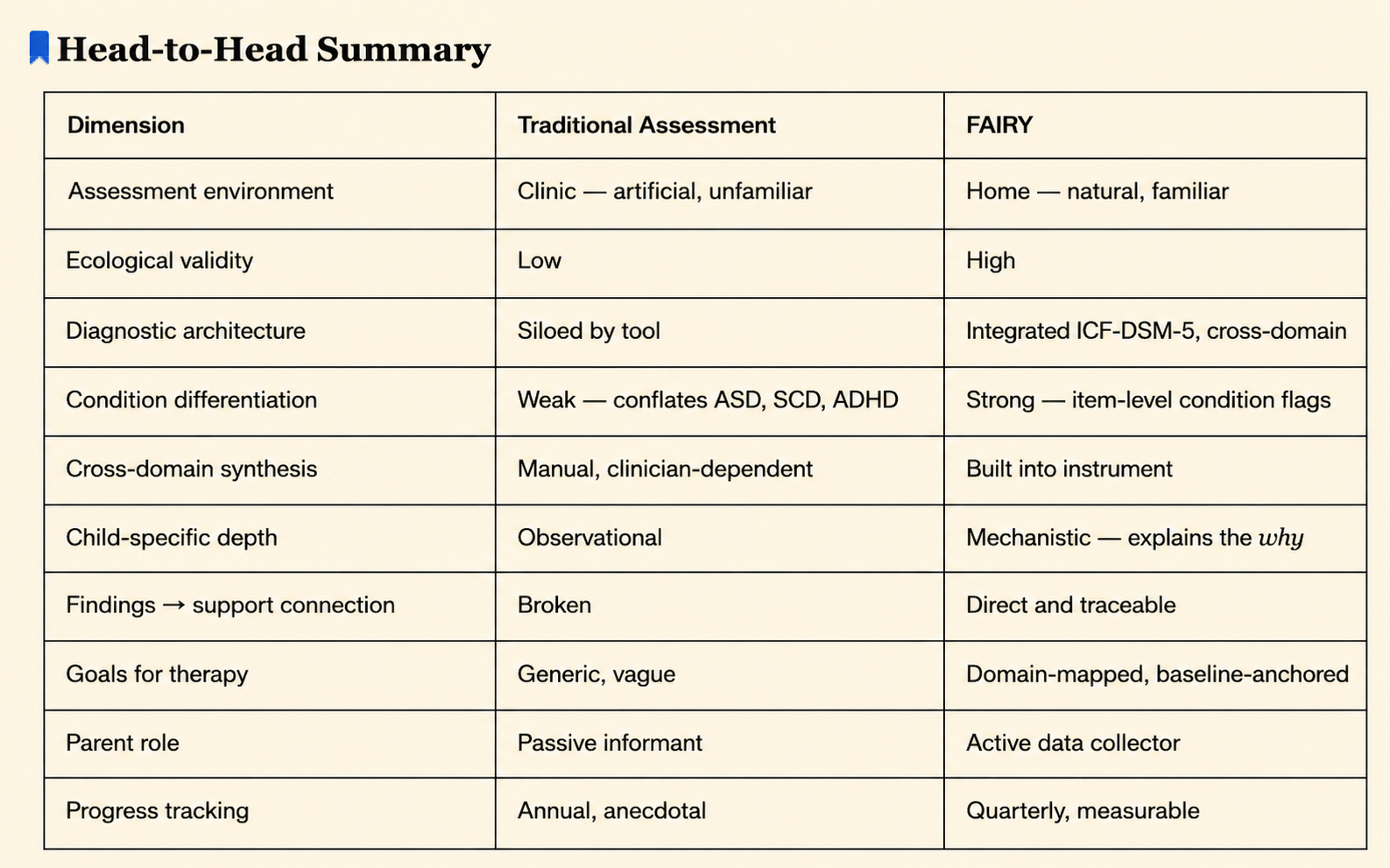
FAIRY vs. Traditional Assessment
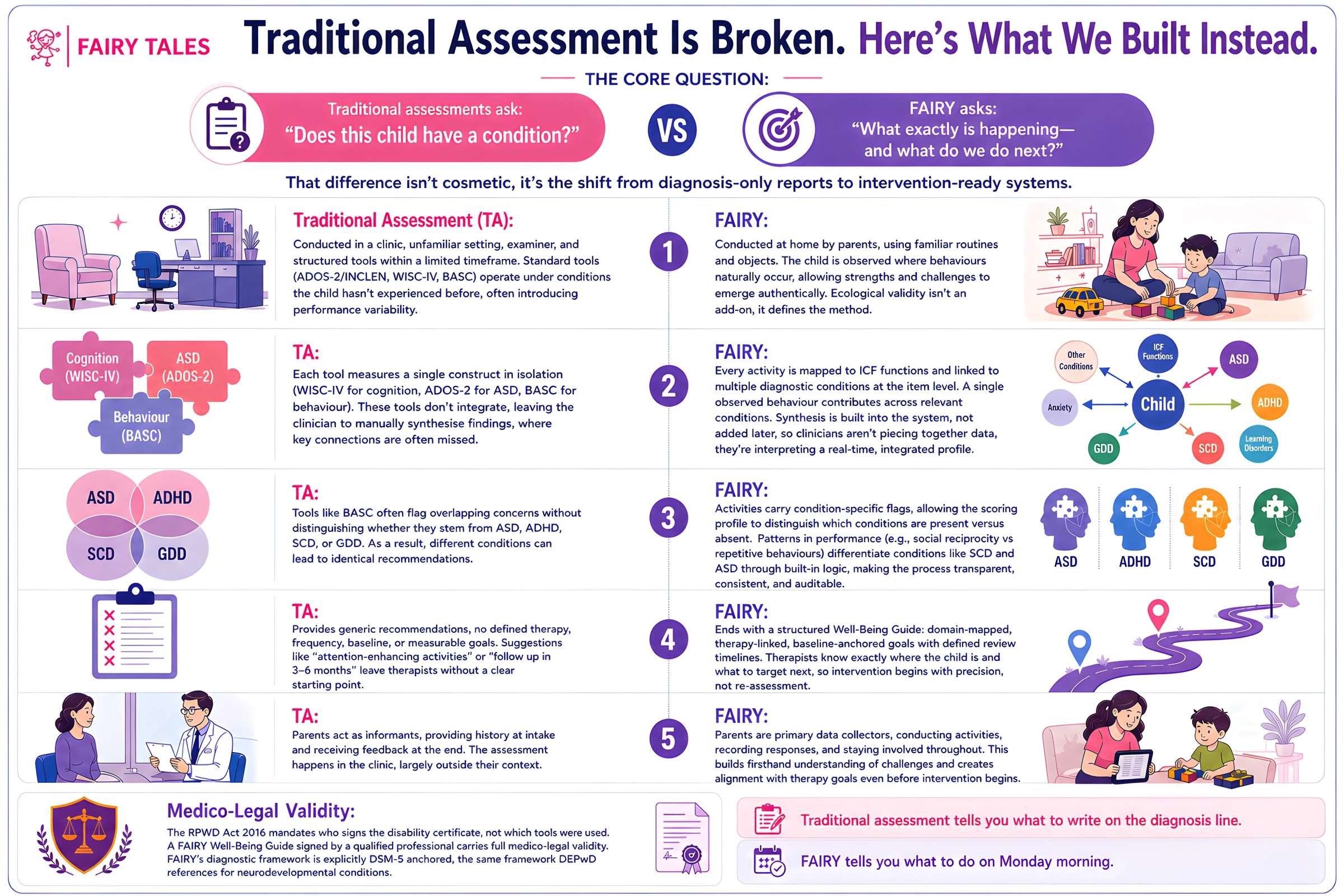
The Core Question:
Traditional assessments were designed to answer:
"Does this child have a condition?"
FAIRY is designed to answer:
"What exactly is happening with this child, and what do we do about it tomorrow?"
That distinction is not cosmetic. It is the difference between a report that ends at diagnosis and a system that begins at intervention.
Where the Assessment Happens:
Traditional Assessment:
A child is brought to a clinic, an unfamiliar room, unfamiliar examiner, structured props, a single day. The ADOS-2/INCLEN observation, WISC-IV administration, and BASC parent-report all happen under conditions the child has never encountered. Clinicians know this introduces performance variability, a child suppressed by novelty or anxiousness in a clinical setting will present differently than they do at home or school. The assessment captures one behavioural snapshot under artificial conditions.
FAIRY
Activities are conducted at home, by a parent, with objects the child already knows, their tricycle, their blocks, their usual mealtime. The child is observed in the environment where their challenges and strengths are most honestly expressed. When a child's ability to adapt to an unexpected change is tested by the parent shifting a feeding location, that is the child's real flexibility being measured, not a performance for a stranger in a room. Ecological validity is not a bonus feature here. It is the methodology.
How Conditions Are Identified:
Traditional Assessment:
Each tool targets one construct in isolation. The WISC-IV measures cognition. The ADOS-2 measures autism features. The BASC captures parent-reported behaviour. These instruments do not speak to each other, the clinician performs the synthesis manually at the end, which is where most diagnostic nuance is either made or lost. A below-average Working Memory score never gets connected to a presenting complaint of reading and writing difficulty, because no instrument in the battery is designed to make that bridge.
FAIRY
Every activity is pre-mapped to ICF functional codes and simultaneously flagged against 8 diagnostic conditions at the item level. When a child fails Response to Joint Attention, that data point automatically contributes to ASD, ADHD, and SCD profiles concurrently, because the architecture knows which conditions share that marker. The synthesis is not done after the assessment. It is built into the instrument. A developmental paediatrician reviewing FAIRY output is not reconstructing a picture, they are reading one that was assembled in real time.
Condition Differentiation:
This is where traditional assessments show their most significant clinical weakness.
Traditional Assessment:
A standard BASC can flag a child as "At Risk" on Functional Communication, Social Skills, and Withdrawal, findings clinically consistent with ASD, ADHD, Social Communication Disorder, or GDD, without making any attempt to differentiate. The recommendations are identical regardless of which condition is driving the profile. A child with ASD and a child with SCD can leave the same clinic with the same bullet points.
FAIRY:
Because activities carry condition-specific flags, the scoring profile differentiates which conditions are active versus which are absent. A child who scores poorly on social reciprocity activities but adequately on rigidity and restricted/repetitive behaviour activities produces a profile that distinguishes SCD from ASD, not by clinician intuition, but by instrument design. The diagnostic logic is transparent, auditable, and consistent across every child assessed.
What the Report Does After Diagnosis:
Traditional Assessment:
Generic recommendations. No therapy modality named. No frequency specified. No baseline established. No measurable goal stated. Recommendations such as "attention enhancing activities", "social skills programs", and "follow up every 3-6 months" give a therapist nothing to work with on Day 1. The parent leaves the clinic with a diagnosis and a direction, not a plan.
FAIRY:
The Well-Being Guide closes with a goals table, domain-mapped, therapy-assigned, baseline-anchored goals with a named review date. A speech therapist picking up this report knows the child is at "single words/phrases" and the goal is "extended conversation." An OT knows the child shows "no gesture use beyond pointing" and the target is "spontaneous, varied gesture initiation." Therapy begins with precision, not re-assessment.
The Parent as a Clinical Partner:
Traditional Assessment:
Parents are informants. They answer historic questions at intake and are counselled at the end. The assessment happens to the child, in front of the clinician, away from the parent's world.
FAIRY:
Parents are the primary data collectors. They conduct the activities, record the responses, and are present throughout. This does two things that traditional assessment cannot: it gives parents firsthand understanding of why a goal exists, because they watched it fail, and it builds therapeutic alliance before therapy even starts. A parent who has personally observed their child unable to initiate joint attention does not need to be convinced that social therapy is necessary. They have seen it.
With FAIRY, assessment is not just about knowing the condition, it's more about understanding the areas that are in need of support for the child.
